1.The rotator cuff and subacromial impingement
4. Arthroscopic subacromial decompression (ASD)
What are the indications for Arthroscopic Subacromial Decompression?
Arthroscopic subacromial decompression is used to treat subacromial impingement pain which fails to respond to non-operative measures such as an injection and physiotherapy. The aim is to create more room for the tendons in the narrow subacromial space by removing inflamed bursal tissue and any bony spurs.
What does Arthroscopic Subacromial Decompression involve?
Two or three small incisions (about 10mm each) are made around the shoulder. Before performing the decompression, a thorough arthroscopic inspection of the shoulder joint is carried out to look for any small tears. If a small partial thickness cuff tear is found, this is pared back to healthy tendon.
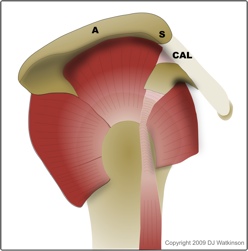
Bony spur(S) on the undersurface of the acromion(A) extending into the coraco-acromial ligament (CAL)
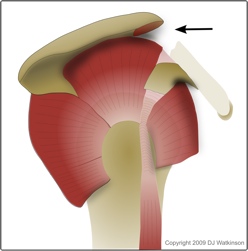
CAL is released and the spur is removed.
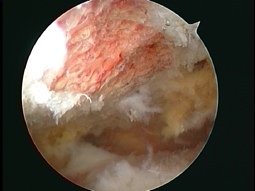
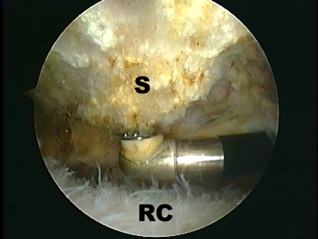
In order to perform the actual subacromial decompression, the telescope is transferred into the subacromial space to view the top surface of the rotator cuff and the undersurface of the acromion. Any inflamed or thickened tissue (bursitis) overlying the tendons is removed with a special arthroscopic shaver and the coraco-acromial ligament is released to expose the front of the acromion. The undersurface of the acromion is then smoothed with an arthroscopic burr and the acromial spur is removed. Finally the front of the acromion is gently bevelled upwards to abolish any friction against the rotator cuff (RC).
One or two stitches are used to close the small skin incisions. These are removed after two weeks.
What sort of anaesthetic will I have?
Arthroscopic subacromial decompression is performed under general anaesthetic (you will be asleep).
The anaesthetist may also recommend a nerve block to numb your shoulder post-operatively. Alternatively, local anaesthetic may be injected into your shoulder at the end of the operation.
What happens after the operation?
Once you are awake, you will be transferred back to the ward.
You will be encouraged to move your arm and shoulder straight away and the physiotherapist will show you exercises to work on your range of movement. It is vital that you perform these regularly (at least three times a day) in order to minimise stiffness.
A sling is not usually required.
You will usually be able to go home the same day.
What happens after I go home?
You will be given pain killers to take home. Please bear in mind that the effects of the nerve block or local anaesthetic will wear off after 8 to 24 hours. It is therefore a good idea to start taking pain killers before the shoulder starts to become sore (about six hours after the operation).
Post-operative physiotherapy is an important part of your recovery. As well as the exercises the ward physiotherapist has shown you, you will also need out-patient physiotherapy. The physio will initially reinforce the range of movement exercises and then gradually introduce strengthening exercises for the rotator cuff and the muscles which contol the shoulder-blade (scapular stabilisers).
By six weeks, your shoulder movement should have more or less returned to normal, but your shoulder may still be a little bit achey. It can take several months for this to settle completely.
When can I go back to work?
This depends on how physical your work is. You will need a minimum of two weeks off, but I would normally recommend a little longer, especially if you have to drive any distance to work. If your job is relatively heavy, then six to eight weeks is usually the minimum, though you may be able to go back on light duties before this.
When can I drive?
Legally, you need to be able to drive in full control of your vehicle. This usually means somewhere between two and six weeks.
It is obviously a good idea to start with short distances and gradually build up.
When can I go back to sport?
This depends on the sport. You should be able to do sports which do not place too much strain on the shoulder within four to six weeks. However throwing or overhead sports (eg: tennis or swimming freestyle) should be reintroduced much more gradually. Your physiotherapist will be able to tailor your rehabilitation program accordingly as it is important to have regained good strength of the rotator cuff and scapular stabilisers before returning to these sports.
What are the risks?
As with any operation, there is a small chance of infection, nerve damage, or bleeding. However with key-hole surgery this risk is very small.
The main risk is post-operative stiffness, which is why it is important to get the shoulder moving straight away. Movement is usually more or less back to normal by six weeks, but it may take longer and a small number of people may develop a post-operative frozen shoulder which can prolong recovery significantly.